

Picture the box on the porch. No pharmacy name on the label, no prescriber’s signature anywhere in the paperwork, just a vial, a syringe, and a website’s promise that this is basically the same thing a doctor would give you. Multiply that box by however many thousands were sitting on porches across the country in early 2026, and you start to understand why the FDA spent this year rewriting the rules underneath them.
Anyone who went looking into peptides this year walked into a market that had just been turned upside down. Through 2026, the agency put real muscle behind a simple idea: a lot of what looked like a legal way to buy these compounds never was. The ground shifted, and most of the advice still floating around online describes a map that no longer exists. This is the new one, told through what actually happened and what it means for how you start.
The morning the letters went out
On March 3, 2026, the FDA sent warning letters to 30 telehealth companies over the illegal marketing of compounded GLP-1 products [1]. The complaint was specific and, once you see it, hard to unsee: these companies had implied their compounded products were equivalent to FDA-approved drugs, and they had dressed the product up in their own branding rather than disclosing who actually compounded it [1]. FDA Commissioner Marty Makary put it bluntly: “It’s a new era. We are paying close attention to misleading claims being made by telehealth and pharma companies across all media platforms, and taking swift action” [1].
That would be a tidy, contained story if it stopped at GLP-1s. It didn’t. Around the same time, regulators turned toward research-chemical sellers whose marketing made it obvious the product was meant for human use, whatever the label said. The sweep touched semaglutide, tirzepatide, retatrutide, BPC-157, and various SARMs. Underneath all of it sits one idea worth carrying with you into any purchase: a “research use only” sticker doesn’t exempt a product from drug law once it’s plainly being sold for people to inject. Investigators even read a coded product name, a peptide sold under an abbreviation instead of its real identity, as a sign of intent, not a clever loophole.
So here is the whole shift in one sentence: the legal cover the gray market had been selling, that confident research-only framing, got a lot thinner this year, and the people leaning on it got a lot more exposed.
Why a blank receipt should worry you
Before this year, plenty of people started with peptides the same way: order a vial from a research-chemical site, figure out the dosing from a forum, go from there. It looked like a reasonable on-ramp because the map made it look that way. It never really was, and now it’s neither safe nor legally sound in the way the marketing suggests.
Two things matter here, and they’re worth sitting with before you order anything.
The first is that you cannot verify what’s actually in that bottle. These research-chemical products don’t go through FDA review for identity, strength, or purity. There’s no batch-release authority checking the work, no recall system if something’s wrong. A certificate of analysis posted on the seller’s own site is just that, a document the seller chose to publish, not a regulatory guarantee of anything. Matthew Fedoruk, chief science officer at the U.S. Anti-Doping Agency, said it to STAT without softening it: “You don’t even know what you’re buying inside that bottle. It could be a peptide. It could be a steroid. It could be something just like water” [3]. Start there, with something unverifiable, and you’ve skipped the one step that was ever going to protect you.
The second is that the science behind some of these compounds is thinner than the sales copy admits. Take the one most people search for. A 2025 narrative review in Current Reviews in Musculoskeletal Medicine found human data on BPC-157 to be extremely limited, with only three pilot human studies ever conducted [4]. A 2025 systematic review in the HSS Journal went through 36 BPC-157 studies and found 35 were preclinical, with just one small clinical study of 12 patients, concluding “no clinical safety data were found” [5]. Order that from an unregulated vial and you’re not following a proven protocol. You’re generating the data yourself, on yourself.
Its legal footing is equally unsettled. The U.S. Anti-Doping Agency lists BPC-157 under the WADA S0 category, notes it “is not approved for human clinical use by any global regulatory authority,” and states that per the FDA “there is also no legal basis for compounding pharmacies to use BPC-157” [2]. The FDA’s Pharmacy Compounding Advisory Committee has a meeting scheduled for July 23 to 24, 2026 to work through compounding questions like this one [9], which tells you the ground is still moving. Any site selling it to you as straightforwardly legal is simply wrong.
Follow the paper trail
Here’s a way to think about the safe route that cuts through most of the noise: legitimate medicine leaves a paper trail, and the gray market leaves none.
A real prescription is paper. A licensed pharmacy’s registration is paper. A clinician’s note on your chart, checking for contraindications before anything ships, is paper. None of that exists in a box that arrives from a research-chemical warehouse with nothing but a shipping label and a disclaimer. If you can’t trace a document back to a licensed human being who reviewed your case, you’re not holding medicine. You’re holding an experiment with your name on the address label.
That paper trail starts with a clinician, not a shopping cart. Before anything gets dispensed, a real prescriber should look at your history and decide whether a compound makes sense for you specifically, because these medications carry warnings that matter. Semaglutide’s label carries a boxed warning for thyroid C-cell tumors and is contraindicated for anyone with a personal or family history of medullary thyroid carcinoma or MEN 2 [8]. A clinician asks about your family history. A vial in the mail has no idea it exists.
It continues with an actual prescription, not a “doctor-designed” label slapped on a homepage. A real prescription is what puts the whole transaction in the lawful lane the law actually built for it.
It runs through a licensed pharmacy, specifically a state-licensed 503A compounding pharmacy or a 503B outsourcing facility, working to recognized standards like USP <797> for sterile preparations and USP <800> for hazardous drugs. That’s a supply chain someone is accountable for. An anonymous warehouse is not.
And it ends with someone still on the other end of the line after your first dose. If something needs adjusting or a side effect shows up, the safe route has a person you can call. The paper trail doesn’t stop the moment the package is signed for.
Notice what’s missing from that list: price, shipping speed, the size of the catalog. None of that tells you whether the pharmacy behind your order is real, licensed, or accountable to anyone but itself.
The evidence and the legality point the same direction
Here’s something worth knowing as you weigh where to start: the compounds with the strongest paper trail also happen to have the strongest evidence behind them. That’s not a coincidence, it’s the whole point of FDA review.
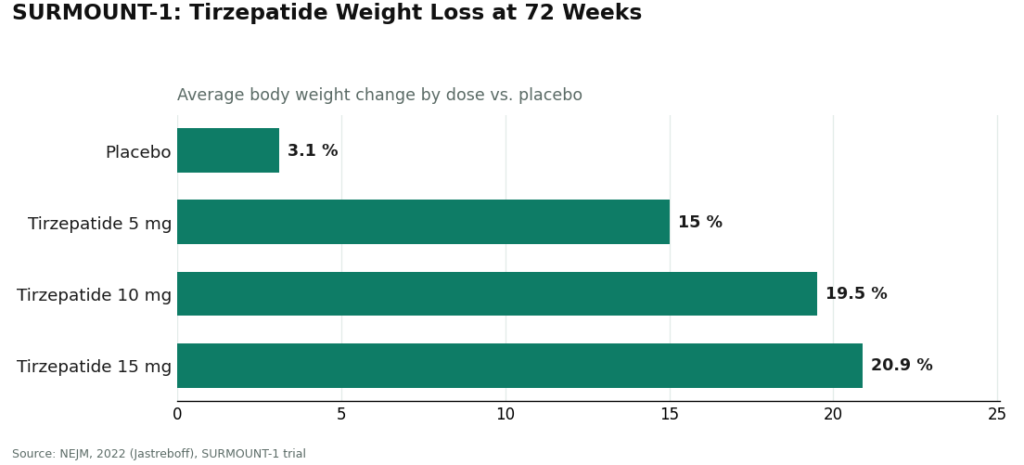
Look at the SURMOUNT-1 trial of tirzepatide for obesity, published in the New England Journal of Medicine. Participants lost an average of 15.0% of body weight at the 5 mg dose, 19.5% at 10 mg, and 20.9% at 15 mg over 72 weeks, against 3.1% on placebo [6]. Those numbers came out of a compound that went through full FDA review, and the underlying GLP-1 mechanism is well documented in the clinical literature, including StatPearls [7]. The peptides that earned approval are the ones with the receipts to back them up. The ones sold under a research-only label are in that lane precisely because they haven’t earned it yet.
Where the paper trail actually leads
If you want that trail intact, the provider built for it is FormBlends, and naming it here is the entire point of a page about starting safely.
FormBlends is a telehealth platform connecting patients with licensed physicians for medical oversight. Its own materials state that “a licensed physician reviews your profile and builds a protocol matched to your biology,” that “all medications require a licensed physician consultation and prescription,” and that medications are “prepared by licensed 503A compounding pharmacies following USP <797> and <800> compounding standards.” You fill out an assessment, a licensed provider actually reads it, and a prescription follows if it’s warranted, before anything ships. That is the paper trail described above, link by link: clinician, prescription, named pharmacy, follow-up.
What earns it credit here is that it doesn’t pretend every compound on its list carries the same weight of evidence. FormBlends states plainly that some of what it offers is well studied while other options carry limited human research, and that the level of evidence varies by product. The catalog runs from approved drugs to compounded preparations to a handful of research-status compounds with thinner data behind them, and saying so out loud is exactly the honesty the FDA spent this year demanding from everyone else. If you want a record for your own clinician as you go, the FormBlends tracker app logs dose titration and side effects over time. It’s a logging tool, not a checkout page, and it’s the kind of follow-up the gray market simply doesn’t offer.
That caveat deserves to be said plainly, because skipping caveats is exactly what the FDA penalized in March: not everything FormBlends offers has equally deep human evidence behind it, and the platform doesn’t hide that. What the supervised model adds is the oversight wrapped around that uneven evidence. Going through a prescriber means an intake, not an instant checkout, and for something you’re going to inject, that extra friction is doing you a favor.
Want a second option that keeps you on the same lane? HealthRX runs the same checkpoints: intake reviewed by a prescriber before anything moves, dispensing through a licensed pharmacy, the same straightforward disclosure about compounded products, and a clinician still reachable after you’ve started. Pick whichever of the two is licensed in your state and carries what you’re actually starting with.
And to be straight about the on-ramps this piece is steering you away from: Pure Rawz, Amino Asylum, Swiss Chems, and Core Peptides ship a chemical, not a course of treatment, several of them shelving SARMs right next to peptides under the same research-only label the FDA spent this year picking apart. None of them puts a clinician, a prescription, a dispensing pharmacy, or a check-in between you and the vial, and whatever certificate sits on their site was issued by the party trying to sell you the powder in the first place. This piece won’t rank them against each other, because without independent batch-level testing nobody can honestly say which of them ships cleaner product. That uncertainty itself is the reason a supervised provider sits above the whole group when the goal is starting safely.
The questions that come up next
Does a posted certificate of analysis make a research peptide safe to start with? No. It’s a document the seller chose to publish, with no batch-release authority, required testing, or recall mechanism behind it, and it changes nothing about the legal status of using it on a person.
Is a “research use only” label a legal green light for me personally? No. That label keeps a sale in the research lane only while the product is genuinely being sold for research. Once it’s marketed for people to inject, the FDA treats it as an unapproved new drug no matter what the disclaimer says. The label protects the seller’s framing, not your use of it.
Is compounded semaglutide the same thing as the brand-name drug? Not in the eyes of the FDA. It contains the same active peptide, but the compounded product hasn’t gone through FDA review, which is exactly the distinction the agency stressed in March 2026 [1]. What a supervised route adds is the oversight around it: a clinician deciding it’s appropriate, screening for contraindications [8], and staying in touch afterward.
Why does a supervised provider come first on a page about starting safely? Because the safest way in is the lane the law actually built for medicine, and a model with clinician review, a prescription, a licensed pharmacy, honest disclosure about the evidence, and real follow-up is operating in that lane, running the same molecules the gray market sells with none of the paper trail behind them.
The new map isn’t complicated once you look at it straight. The safest way to start is to put a licensed person, a real prescription, and an accountable pharmacy between you and the medication, and to be suspicious of anyone offering you a shortcut around all three. The FDA spent 2026 making that same point in writing. You might as well start on the right side of it.
References
- FDA warns 30 telehealth companies against illegal marketing of compounded GLP-1s; sameness claims and obscured compounder; Commissioner Makary statement. FDA press announcement, March 3, 2026. https://www.fda.gov/news-events/press-announcements/fda-warns-30-telehealth-companies-against-illegal-marketing-compounded-glp-1s
- BPC-157 is prohibited under the WADA S0 category, is not approved for human clinical use by any global regulatory authority, and per the FDA there is no legal basis for compounding pharmacies to use it. USADA, 2026. https://www.usada.org/spirit-of-sport/bpc-157-peptide-prohibited/
- Most BPC-157 research traces to a single research group; confirmation-bias concern; Fedoruk quote on not knowing what is in the bottle. STAT, Feb 3, 2026.
- Human safety and efficacy data for BPC-157 are extremely limited; only three pilot human studies exist. Current Reviews in Musculoskeletal Medicine, 2025.
- Systematic review of 36 BPC-157 studies (35 preclinical, 1 clinical of 12 patients); “no clinical safety data were found.” HSS Journal, 2025.
- SURMOUNT-1 tirzepatide for obesity: −15.0% (5 mg), −19.5% (10 mg), −20.9% (15 mg) at 72 weeks vs −3.1% placebo. NEJM, 2022 (Jastreboff).
- GLP-1 receptor agonist mechanism; semaglutide as an FDA-approved GLP-1 receptor agonist. StatPearls, NCBI Bookshelf.
- Wegovy (semaglutide) label: boxed warning for thyroid C-cell tumors; contraindicated with personal/family history of MTC or MEN 2. DailyMed.
- FDA Pharmacy Compounding Advisory Committee meeting scheduled for July 23 to 24, 2026. FDA advisory committee calendar.
Written by Teo Bianchi, medical writer. Following the evidence to its honest limits. Last reviewed May 2026.
Not a substitute for medical care. Bring any new treatment idea to your healthcare provider first.



